
Unions are key to high-quality public education
Our recent report asks a bold question: What would the United States look like if we tripled union membership? We find a range of economic and social benefits—such as higher wages, greater access to health insurance, and a stronger democracy. This post examines another social good generated by unions: strong investment in public education.
Investment in public education was one of the key reasons the U.S. became the richest country in the world in the 20th century. Universal education has many positive effects, including creating a more productive workforce and a more informed and engaged democratic society. Unions play a key role in advocating for public spending in education. Figure A shows that states with higher unionization rates spend substantially more per student on education.
Figure A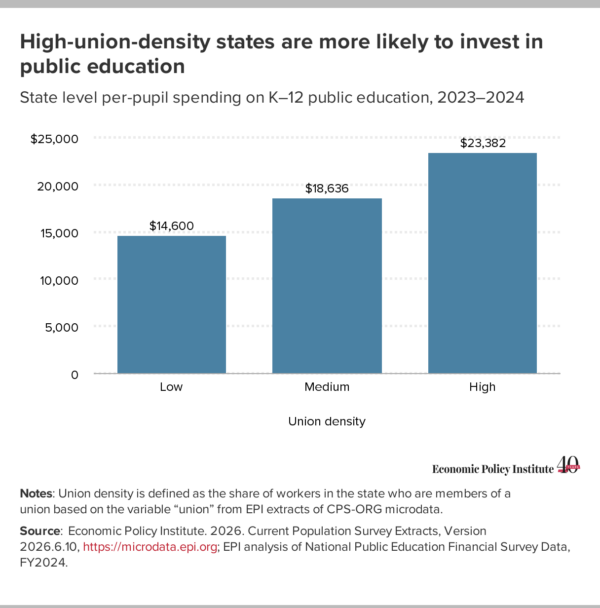
Adequate levels of per-pupil spending are instrumental policy for maintaining quality education. When per-pupil spending is low, students may struggle to get the support they need to achieve their learning goals. Districts, in turn, may have a harder time retaining teachers and staff because they can’t offer competitive salaries or benefits.
Increased per-pupil funding, by contrast, pays off for students. Greater funding for schools improves educational attainment, student achievement, and economic outcomes in adulthood. In one study, researchers found that a 10% increase in school spending for 12 years led to increases in high school graduation rates, 7% higher wages, and 10% higher family incomes in adulthood for children from districts that experienced the spending increase. More recently, researchers assessing the contribution of federal pandemic educational aid found that each $1,000 increase in per-pupil spending boosted student achievement in math and reading. Importantly, when researchers restricted their assessment to high-poverty districts, the per-dollar effect was nearly twice as large.
Unions are also instrumental to protecting quality public education. This is increasingly under threat due to state- and national-level voucher programs, which divert money away from public education and toward private schools and homeschooling. A substantial share of enrollees in voucher programs are often students who are already attending private school.
Vouchers reduce education quality in several ways. First, voucher programs yield worse academic achievement outcomes relative to public schools. Studies have found that students in voucher program schools experienced test score declines that are comparable or worse than declines due to COVID-19.
Second, voucher programs strain state budgets. And this cost comes at a time when states face budgetary pressure from the Republican tax and spending megabill (OBBBA), which reduced federal funding for Medicaid and SNAP (also known as food stamps).
Third, public school districts experience an additional hidden cost. When students leave public schools with a voucher, school districts lose revenue but must still pay the same amount for fixed costs that can’t immediately adjust to declines in enrollment, such as cooling/heating and utilities. These required payments for a district’s fixed costs mean that districts will have even less to spend on costs that can be adjusted—like school supplies or instructional support—thereby reducing services for students.
States with higher levels of unionization are more likely to have the political resources to fight back against vouchers in legislative fights. As a result, these states are less likely to have universal voucher programs, as shown in Figure B.
Figure B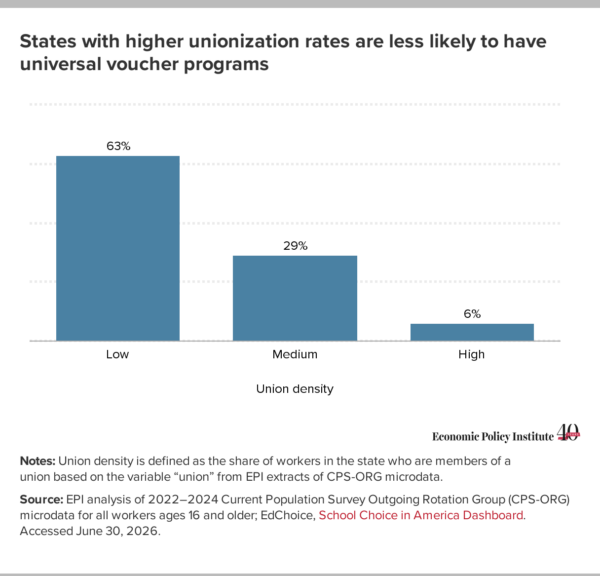
In sum, there are many ways unions support workers and their communities, and their consistent support of public education shouldn’t be discounted. From advocating for enough funding for high-quality education to defending against education privatization, unions support our nation’s commitment to universal public education. This not only improves students’ academic achievement, but also their economic outcomes well into adulthood.
Recent comments